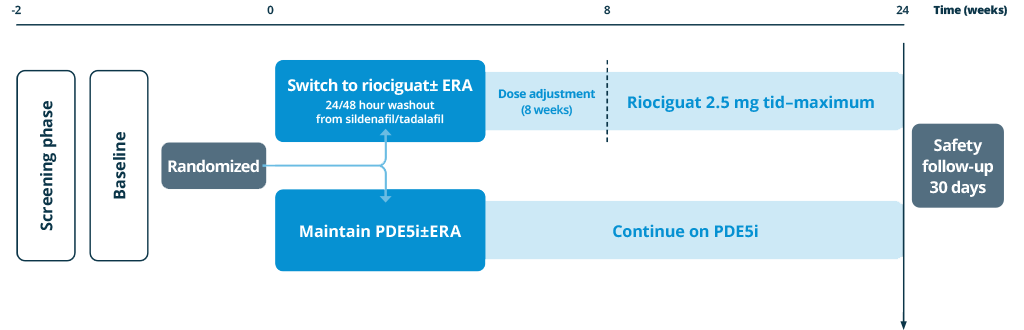
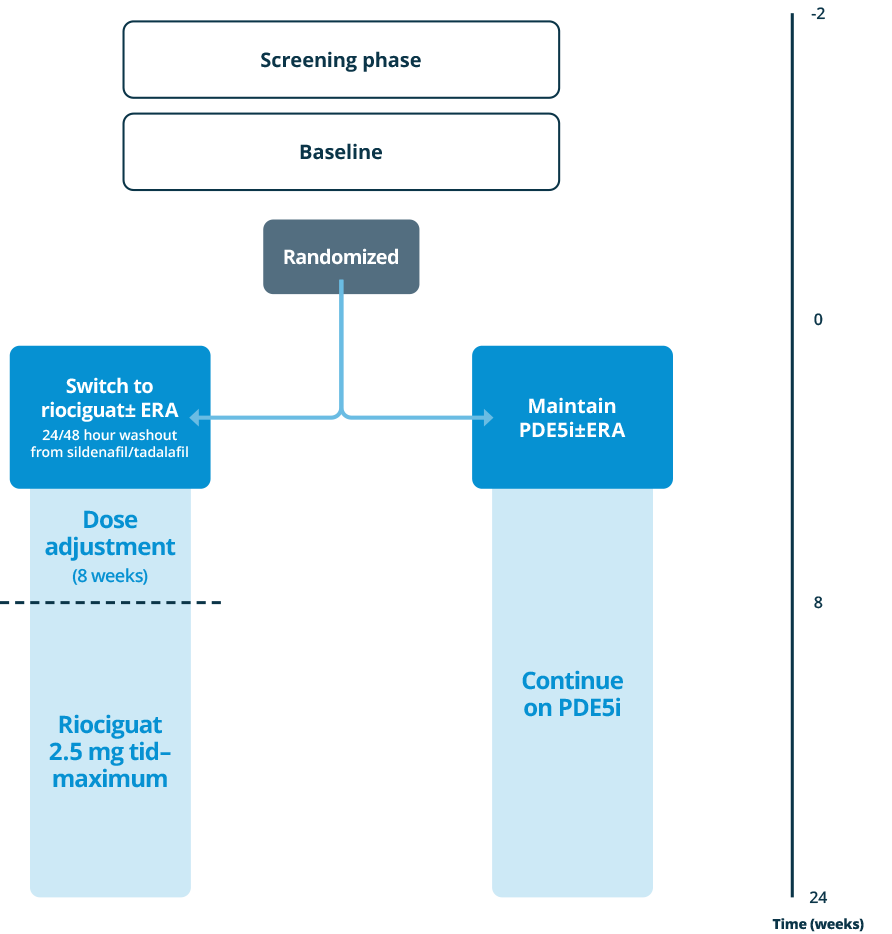
A prospective randomized, international, multicenter, double-arm, controlled, 24-week open-label Phase IV study assessing the effect of switching to riociguat compared with maintenance of stable PDE5iPDE5i: phosphodiesterase type 5 inhibitor in patients with PAHPAH, pulmonary arterial hypertension at intermediate risk.